Global Online Journal of Academic Research (GOJAR), Vol. 2, No. 3, May-June 2023. https://klamidas.com/gojar-v2n3-2023-01/ |
||||
|
Reachability and Uptake of Modern Contraceptives among Spouses in Kogi State, North-Central Nigeria By Edward Ukwubile Egwuaba & Sunday Blessing Adeyi Abstract This study investigated the reachability and uptake of modern contraceptives among spouses in Kogi State, North-Central, Nigeria. Specifically, amongst others, it determined how the level of reachability of modern contraceptives affect the use among spouses in Kogi State, and identified those factors that affect the use of modern contraceptives among spouses in Kogi State. The study made use of five theories, but relied on the rational choice theory in explaining the social phenomena studied. The study adopted cross-sectional survey design. Kogi State has a 2016 projected population of 4,473,490. However, the population for the study consisted all spouses of age 18-49. The study has a sample size of 1067. The instruments for data collection were questionnaire, in-depth interviews (IDIs) schedules and Focus Group Discussion (FGD) guide. Multi-stage sampling techniques, entailing simple random sampling, systematic and purposive sampling techniques, were adopted in the study. The data analysis was based on 1,064 questionnaires that were correctly filled and returned by the respondents out of the 1067 distributed. A total of 6 IDIs and 12 FGDs were conducted in the study. Descriptive statistics like frequencies and percentages were employed in interpreting the data, while chi square was used in testing the hypotheses. Results revealed that 50.3% of the respondents report non availability of modern contraceptives in their locality which affects contraceptives use among spouses in Kogi State. 75.2% of the study respondents report that lack of education amongst majority of spouses as well as several other determinants like non-accessibility, cost, proximity or distance of clinics from their homes and religion and culture of the people account for poor and low use of modern contraceptives in Kogi State. Based on the above findings, the study recommends that sociologists should educate and create more awareness about the need of spouses to use modern contraceptives by organizing programmes that educate and keep spouses and reproductive persons well informed. Government should collaborate with international bodies and organizations that are capable of providing the required healthcare needed by spouses that can provide these services at subsidized rate for spouses. If possible, government should incorporate and implement already formulated policies that promote free family planning services to rural dwellers. Keywords: reachability, modern contraceptives, Kogi State, healthcare, family planning
Introduction The growing use of modern contraceptives around the world has given spouses the opportunity to control the number of children they give birth to, in addition to other tremendous lifesaving benefits. The availability of family planning services allows individuals to achieve desired birth spacing and family size, and contributes to improved health outcomes for infants, children, women, and families (Center for Disease Control and Prevention [CDCP, 1999]; Gipson, Koening & Hindin, 2008; Sonfield, Hasstedt & Gold, 2014). Access to safe, voluntary family planning is a human right. Family planning is central to gender equality and women’s empowerment, and it is a key factor in reducing poverty (Guttmacher Institute, 2014; Gavin & Pazol, 2016; Lawrence & Mia, 2016). Yet in developing regions, an estimated 218 million women who want to avoid pregnancy are not using safe and effective family planning methods, for reasons ranging from inadequate access to information or services to lack of support from their partners or communities (Gavin, Moskosky & Cater, 2014). This threatens their ability to build a better future for themselves, their families and their communities (Berghella, Buchanan & Pereira, 2010). However, despite the campaign on the usefulness of family planning in having smaller and healthier family, studies by National Population Commission (2009) and Adeleye, Akoria, Shuaib, & Ogholoh (2010) indicate that contraceptive use is still low in many developing countries, including Nigeria and Kogi State, where only 24 percent and 8.5 percent of currently married women had used one method of contraceptive. Different factors such as culture, low education, poverty and poor access to contraceptives, among others, have been identified by scholars as issues militating against the use of contraceptive methods (Bankole, 2008). Monjok, Andrea, John, & Essien (2010) argue that the rate is very low, despite high rate of sexual activity and wide spread knowledge of contraceptive methods particularly among young couples, leading to unintended pregnancies and illegal abortions. Though a number of studies have been done in some other parts of Nigeria on access and use of modern contraceptives among couples of reproductive ages, none has been on the availability and use of modern contraceptives among spouses in Kogi State. Although the state boasts of about 247 family planning clinics, it has the lowest adoption rate within the middle belt region – about 11 percent for any contraceptive method, 8.5 percent for modern methods. This necessitated the present study in other to fill this gap. Statement of the Problem The present population of the world is about 7.9 billion people with four-fifth of them living in the developing societies and keeps increasing by 90 million annually, with 90 percent of the increase occurring in developing societies. This is because population growth rate in developed societies is considerably lower than in developing societies. In the past, the need for family planning had been rationalised by a significant number of women who state a desire to stop childbearing. However, because of unmet needs for contraceptives, very little has been achieved in aggregate fertility reduction. This trend in the uptake of family planning services has not spared Kogi State in general where there is large estimated number of births per household (Kogi State Economic Empowerment and Development Strategy [KOSEEDS], 2015). Standards of living tend to worsen when the rate of population growth exceeds the rate of economic growth. At the household level, the high fertility rate may be contributing towards depletion of productive resources in the society, rising cost of living, ill health, poor nutrition and limited educational opportunities, ultimately trapping women and families in poverty cycle. Moreover, considering the young age structure of West African, the number of women of reproductive age is expected to increase population growth and challenges to meet the different needs of these people (Nabila, 2014; Adensi-Pipim, Kwafo, & Garchiner, 2016). The combination of high fertility and a growing number of women of reproductive age sets the stage for continued rapid population growth. Objectives of the Study Specifically, this study was undertaken to:
Review of Related Literature The concept of family planning Family planning has attracted attention all over the world due to its relevance in decision making, population control and development. Samuel (2010) defined family planning as the practice that helps individuals or couples to attain certain objectives such as avoiding unwanted pregnancies, bringing about wanted babies at the right time, regulating the interval between pregnancies, controlling the time at which birth occurs in relation to the ages of parents and determining the number of children in the family. Family planning is defined as the ability for individuals and couples to attain their desired number of children and plan the spacing and timing of their births through use of contraceptive methods (WHO, 2013). Family planning utilisation across the globe Several studies have been carried out throughout the world to examine family planning and use among couples and groups. A study carried out by Rugendo and Maseno (2015) on assessing utilisation of family planning services among women of reproductive age in North Kanyabala revealed low usage of contraceptives compared to the national level (53 percent), and use of services varied in terms of level of education and sources of income. Pascal and Ghana Health Services (2014) studied factors influencing the uptake of family planning services in the Talensi District, Ghana, and the results revealed that 89 percent of respondents were aware of family planning services, 18 percent of respondents have used family planning services in the past. Similarly, World Health Organisation Report (2010) on the statistics of contraceptive prevalence in 53 African countries showed that Nigeria has 14.1 percent contraceptive prevalence rate, unlike other African countries like Mauritius with 75.8 percent, Morocco 63.0 percent, Algeria 61.4 percent, Cape Verde 61.3 percent, Egypt 60.3 percent, South Africa 60.3 percent, Tunisia 60.2 percent, Zimbabwe 60.2 percent, Namibia and Swaziland with 55.1 percent and 50.6 percent respectively. Another study by Adinan (2013) on awareness and practices of family planning in Wa Municipality of Ghana revealed that 88 percent of respondents were generally aware of family planning even though family planning practices remained as low as 12 percent. Also, a study by RoumiDeb (2010) on knowledge, attitude and practices related to family planning methods among the Khasi tribes of East Khasi hills Meghalaya, India, showed that the awareness level among Khasi tribe was very high but only half of the women adopted family planning. Reachability and utilisation of family planning services across Africa Many sub-Saharan Africa countries have high rates of unmet need for family planning (FP) (Westoff, 2011; Bongaart, & Bruce, 2012) and low rates of contraceptive use (Bongaart, & Bruce, 2012). Individuals and couples who want to limit their fertility are often unable to obtain the Family Planning methods they need due to numerous barriers (Campbell, Nuriye, & Malcolm, 2006). These barriers include high cost, long distances, poor distribution, medical restrictions and fear of side effects, or even misinformation. Although much of the available literature assumes that financial cost is the primary factor inhibiting contraceptive use, various studies around the world suggest that fear of side effects of FP are more influential in decision-making (Campbell, Nuriye, & Malcolm, 2006; Darroch, Gilda, & Haley, 2011; Colombia Demographic and Health Survey, 2005; Uganda Bureau of Statistics and ORC Marco, 2001; Sedgh, Rubina., Akinrinola, & Susheela, 2007). It is estimated that 59 percent of unintended pregnancies could be eliminated if method-related reasons for non-use were overcome; and fear of side effects is the most commonly cited reason for such non-use (Darroch, Gilda, & Haley, 2011). The fear of side-effects is also a commonly cited reason for contraceptive discontinuation (Bradley, Hilary, & Shane, 2009). Many studies have found that while some of these are based on actual health related side effects, many fears are based on rumours, rather than personal experience (Campbell, Nuriye, & Malcolm, 2006; Schuler, Maria, & Susanna, 1994; Cstle, 2003; Rutenberg & Watkins, 1997; Keesera, 2009; Hall, Stephenson, & Juveker, 2008; Plummer, Wight, Wamoyi, Hayes, & Ross, 2006). A study in Nepal found that side effects were the main reasons cited for discontinuing the use of FP and that most people received information about FP from mass media (Tuladhar & Marahatta, 2008). In Nigeria, knowledge of FP is generally high; however, use remains low. The main reasons for this lack of FP use include fear of complications, lack of understanding of methods and fear of opposition from the husband (Obisesan, Adeyemo, & Fakokunde, 1998). Nadia, Campbell, & Seema (2012) identified evidence of fear of FP side effects among females and males from India, Nepal and Nigeria. Furthermore, fear of side effects from hormonal methods among male partners has also been found to impact females FP decision-making and their fear to use FP (Raine, Jennifer, Cherrie, Sadia, Beth, Hernandez, & Harper, 2010). Generally, researches show that spousal communication can increase contraceptive uptake and continuation (Bawah, 2002; Nzioka, 2002; Sharan & Valente, 2002; Miriam, Kate, Dominik, Brad, & Greg, 2012). Moreover, it is clear that spousal discussion and partner approval are significant in inducing a woman to use modern contraceptives in the Central Terai region of Nepal (Kang, O’ Donnel, & Sparks, 2010). Utilization of Modern Contraceptives/Family Planning Services in Nigeria Several studies have also been conducted to explore family planning services utilisation in Nigeria. Lasisi, Bassey, Ita, & Awoyemi (2014) carried out a study on the awareness and utilisation of family planning among married women in the traditional core areas of Ibadan, Oyo State. Result showed that the utilisation of family planning methods was low among married women in OpoYiosa (9 percent) and Ayeye (11.2 percent), but high in Mapo, Oja-Oba and Inalende with utilisation rates of 31.5 percent, 29.2 percent and 19.1 percent respectively. Also, Obisessan, Adeyemo, & Takokude (1998) studied the level of awareness and the rate of family planning method use among women of reproductive age in Ibadan, Nigeria, on 1188 married women. Result revealed that 94.3 percent were aware of family planning methods, but only 12 percent had visited a family planning clinic. Specifically, the study found that the awareness of specific method was 82.6 percent for condoms, 75.7 percent for oral contraceptives, 75.5 percent for injectable contraceptives and 65.5 percent for IUDs, while current use of family planning methods was low, with 10 percent using withdrawal, 8.1 percent using oral contraceptives, 5.2 percent using IUDs and 4.7 percent using condoms. In another study by Clifford (1999) on family planning attitudes and use in Nigeria, a factor analysis found out that majority of respondents reported knowing a contraceptive method (76 percent), only 28 percent were currently using one, and fewer than half (47 percent) reported ever having used one. Eko, Osonwa, Osuchukwu, & Offiong (2013) in a study in Calabar, Southern Nigeria, on prevalence of contraceptive use among women of reproductive age pointed out a low prevalence rate of contraceptive use of about 21.6 percent. Theoretical Thrust Rational choice theory was propounded by Adam Smith in the 1700s and refers to a set of guidelines that help understand economic and social behaviour (Blume & David, 2008). Rational choice theory (RCT) theorists believe that most human decisions are based on maximizing a person’s own benefits, while minimizing that which can hurt the individual. Rational choice theory proposes that there are two outcomes of two choices regarding human action. Firstly, the feasible region will be chosen within all the possible and related action. Second, after the preferred option has been chosen, the feasible region that has been selected was picked based on restriction of financial, legal, social, physical or emotional restrictions that the agent is facing. After that, a choice will be made based on the preference order (De-Jonge, 2012). The theory postulates that an individual will perform a cost-benefit analysis to determine whether an option is right for them (Gary, Abigail, Frank, 2000). It also suggests that an individual’s self-driven rational actions will help better the overall economy. Rational choice theory looks at three concepts: rational actors, self-interest and the invisible hand (Levin & Milgrom, 2004). The basic premise of rational choice theory is that the decisions made by individual actors will collectively produce aggregate social behaviour. The theory also assumes that individuals have preferences out of available choice alternatives. These preferences are assumed to be complete and transitive. Completeness refers to the individual being able to say which of the options they prefer (i.e. individual prefers IUD over vaginal rings, vaginal rings over IUDs or are indifferent to both). Alternatively, transitivity is where the individual weakly prefers option IUDs over vaginal rings and weakly prefers option vaginal rings over oral contraceptive pills, leading to the conclusion that the individual weakly prefers IUDs over oral contraceptive pills. The rational agent will then perform their own cost-benefit analysis using a variety of criteria to perform their self-determined best choice of action. Rational choice theory does not claim to describe the choice process, but rather it helps predict the outcome and pattern of choice. It is consequently assumed that the individual is self-interested or being homo economicus. Here, the individual comes to a decision that maximizes personal advantage by balancing costs and benefits (Grune-Yanoff, 2012). Rational choice theory can be viewed in different contexts. At an individual level, the theory suggests that the agent (spouses) will decide on the action (or outcome) they most prefer. If the actions (or outcomes) are evaluated in terms of costs and benefits, the choice with the maximum net benefit will be chosen by the rational individual. Rational behaviour is not solely driven by monetary gain, but can also be driven by emotional motives. It is important that in promoting spouses’ access and use of modern contraceptives, medical/health sociologists as well as service providers need to identify such barriers and work with spouses to reduce them. Family planning service providers should help spouses to identify these barriers and help them to reduce it through counselling and prompt use of modern contraceptives. Since every spouse would want to live a healthy life, have healthy babies and a balanced family they are likely to take action that will help them to avoid the risk of unplanned pregnancies and to take necessary intervention so as to manage, plan, and provide for their families adequately, if the benefits are adequately explained to them. The above-mentioned model is selected because it best explains the behaviour and actions taken by spouses towards accessing and using reachable modern contraceptives and its implications on their health. Study hypotheses The following hypotheses were guide to this study:
Methodology This study adopted a multi-stage cluster sampling procedure. This entails successive random sampling, systematic and purposive sampling techniques for the selection of respondents from communities, wards, villages, streets, households and respondents that were involved at the services centres in the study. In the first stage, Kogi State was purposively divided into three in line with the three geo-political senatorial districts. The local governments found in the state represents urban and rural. 14 LGAs to be studied were then randomly selected in the proportion of 3:6:5 from Kogi Central, Kogi-East and Kogi-West senatorial districts respectively based on the 2006 population census result which reflected the population proportion as such. Given a sample size of 1067 respondents, each were assigned respectively to urban and rural areas. To achieve this, the researcher used a list of the enumerated areas (EAs) in each of the fourteen LGAs obtained from the National Population Commission (NPC, 2016), Kogi State, alongside with the population result of 2016 projection. In each of the LGAs, five percent of the EAs were selected using systematic random sampling. Three streets were picked randomly from the EAs from where every 5th household was selected for further sampling. Samples drawn from each of the fourteen LGAs were determined by the proportion of the population of each of the LGA to the overall population of the LGAs selected with a view to ensuring evenness of the samples drawn. The sample size was 1067 drawn from fourteen local government areas out of the twenty-one (21) LGAs in Kogi State and from the total number of households (495,786) that made up each local government from the selected ones. Due to the scattered habitation arrangement in the rural communities, the researcher and his assistants twirled a bottle at the market square and whichever direction the neck of the bottle faced served as the starting point. Two eligible members in each household were purposively selected in each unit taking into account the age variable, and any household that did not have persons (respondents) with the required characteristics were substituted with another household until the desired number of the respondents was achieved. For clearer demonstration, the household that had three or more persons within the age range, two of them were selected using SRS (balloting). Qualitative data was also collected with the use of both In-Depth Interview (IDI) guide and Focus Group Discussion (FGD) guide. The IDI and FGD helped to explore information on availability and use of modern contraceptives among spouses as were expressed by the participants in IDI and FGD sessions. The information derived from IDI and FGD helped to complement the data collected from questionnaire. For the qualitative data, six FGD sessions were conducted in the selected wards and villages of urban communities and rural communities. Each session was made up of between 6-12 participants, aged 18 to 49 years. To achieve this, there were six FGD sessions (one male and one female) in the urban and rural communities of Kogi-Central, Kogi-East and Kogi-West. To select the respondents for the FGD from the two wards that represented urban communities, the researcher liaised with the research assistants who were residents/indigenes of the selected wards to help in selecting the participants for the discussion. Also, to select the respondents for the FGD from the villages that represented rural communities, the researcher liaised with the research assistants who were residents/indigenes of the selected villages to help in selecting the participants for the discussion. The participants for the FGD were purposively selected putting into consideration their age and sex. The researcher facilitated the six IDIs while two of the research assistants served as note takers. The six IDI sessions were conducted in locations, days, and time chosen by the interviewees. Findings/Results Table 1: Distribution of Respondents’ Socio-Demographic Characteristics
Source: Author’s Field Survey, 2022 This current study was carried out in Kogi state, Nigeria. Questionnaires were distributed among three regional districts to elicit information for this study. Data in Table 1 showed that more than half of the respondents were women (59.2%) while men were 40.8%. The reason for this finding can be traced to the fact that most often women are readily available and easily accessible. The study area is highly populated with the women folk, they actively participate in health, community, and religious activities; their readiness to participate fully in this study is shown in their large representation. Respondents’ age intervals indicated that those aged 26 – 33 years were 48.1%, those aged 18-25 years were 27.4%, those aged 42-49 years were 14.6% while those aged 34-41 years were the least sampled (9.9%). The relevance of this finding showed that those within the age interval of 26-33 years are young, are busy occupied with the happenings of life and are always ready to partake in activities that bring about change and development. Hence, their willingness to participate in this study. In terms of respondents’ marital status, the information displayed in Table 1 showed that those who were married (68.5%) were the highest; this is followed by those separated (13.4%). Also, those who were widowed were 10.2% while those divorced were 7.9%. The displayed data in Table 1 revealed that respondents who had their secondary education were 36.7%, those who had obtained their tertiary education were 25.4, and those who had their primary education were 21.0% while those who had no formal education were 17.0%. This finding revealed that citizens of Kogi state have value for education as more than half of the respondents either had their primary, secondary or tertiary education. Furthermore, results on Table 1 showed that civil servants (43.4%) were more in this study. The next to them were those who were unemployed (27.3%). Those who were into trading were 12.2%, those who were artisans were 8.7% while those into farming were 8.4%. The relevance of this finding to this study showed that even if majority of the respondents had obtained their primary, secondary or tertiary education, most of them still struggled with unemployment. Respondents’ monthly income showed that majority (24.2%) of them earned between 41,000-60,000 naira. This is followed by those who earned 61,000-80,000 naira (22.4%). Those who earned 81,000-100,000 naira were 19.7%, those who earned 21,000-40,000 naira were 17.2%, and those who earned less than 20, 000 naira were 10.3% while those who earned above 100, 000 naira were only 6.1%. Two major religions exist in the study area. Results in Table 1 showed the religious affiliation of the respondents. The result revealed that respondents who were Christians accounted for 59.1% while Islam accounted for 40.9%. On family type of the respondents, the results indicated that 68.5% of the respondents were involved in monogamy while only about 31.5% practised polygamy. This finding showed that most persons in the study area are only married to one wife or one husband. The study further enquired about the number of children respondents’ intended or would love to have. Data in Table 4, 13 showed that slightly above half (50.9%) of the respondents desired to have 4 children, 17.1% mentioned that they would love to have 3 children, 16.5% said they would love to have 6 children and above, 12.8% said they would love to have 5 children while only 2.6% of the respondents indicated that they would love to have just 2 children.
Figure 1: Distribution of Respondents on reachability of family planning services in their locality Source: Author’s Field Survey, 2022 The information portrayed in Figure 1 showed responses of the respondents on the availability of family planning services in their locality. Out of the 1064 respondents utilised for this study, 50.3% of the study respondents indicated that their area of location had no available family planning services while 49.7% said that they had available family planning services in their area. This finding implies that despite the high level of knowledge of family planning, majority of the respondents do not enjoy these services since it is not available in their locality.
Figure 2: Distribution of Respondents on access to family planning services Source: Author’s Field Survey, 2022 Data in Figure 2 showed that out of the 1064 respondents used for this study, 54.5% of the study respondents indicated that they had no access to family planning services while 45.5% said they had access to family planning services. This finding implies that not everyone in Kogi state has access to family planning. The problem with accessing family planning services can be traced to distance and locality of the respondents. Data from the qualitative study supports this. According to a female participant: “The family planning centre is quite far from my place of residence and coupled with the hard economic state of things in our state, I find it hard making it to the family planning centre for the use of the services therein” [Participant: FGD; Female, Kogi-East]. Another participant also opined thus: “My place of residence is really far from the family planning clinic but I still manage to go there to get and use the available services to help in planning and spacing my children so as to enjoy good health as well.” [Participant: FGD; Female, Kogi-Central].
Figure 3: Distribution of respondents on current use of modern contraceptive method (n=1064) Source: Author’s Field Survey, 2022 The study sought to find out if respondents were currently utilizing modern family planning method. Data displayed in Figure 3 showed that majority (52.5%) said they were not currently utilizing family planning methods while 47.5% said they were currently utilizing family planning methods.
Figure 4: Distribution of respondents on current modern contraceptives been used (n=505) Source: Author’s Field Survey, 2022 Data in Figure 4 showed the percentage distribution of respondents’ answers to the type of family planning they were currently using. Majority (81.2%) of the respondents mentioned that they were currently using oral contraceptives, 9.7% said they were using condoms, 5.1% said they were using withdrawal method, 2.6% said they were doing periodic abstinence, 1.2% said they were using Billings ovulation method while 0.2% mentioned cervical cap. This finding implies that the commonest type of family planning method employed is the oral contraceptives and this may be as a result of its high level of safety and its accessibility/cost.
Respondents were asked the reasons for their choice of the type of family planning method they are using. Data in Table 2 showed that majority (85.4%) of the respondents said the method was suitable and effective/reliable, 4.7% said it was affordable, 3.85 said it has little side or no side effect, 3.0% said it is readily available, 2.3% said it involves their partner’s usage and .8% had no reason for using the family planning method they are currently using.
Figure 5: Distribution of Respondents on reasons for non-use of contraceptive methods Source: Author’s Field Survey, 2018 In Figure 5, respondents were asked their reasons for not using family planning. Majority (22.6%) of the respondents said it is not easily accessible, 20.3% indicated fear, 20.0% said it is expensive, 18.5% said it encourages promiscuity, 7.8% said it is against their culture, 6.9% mentioned that it is against their religion and 3.9% said it diminishes their sexual activity.
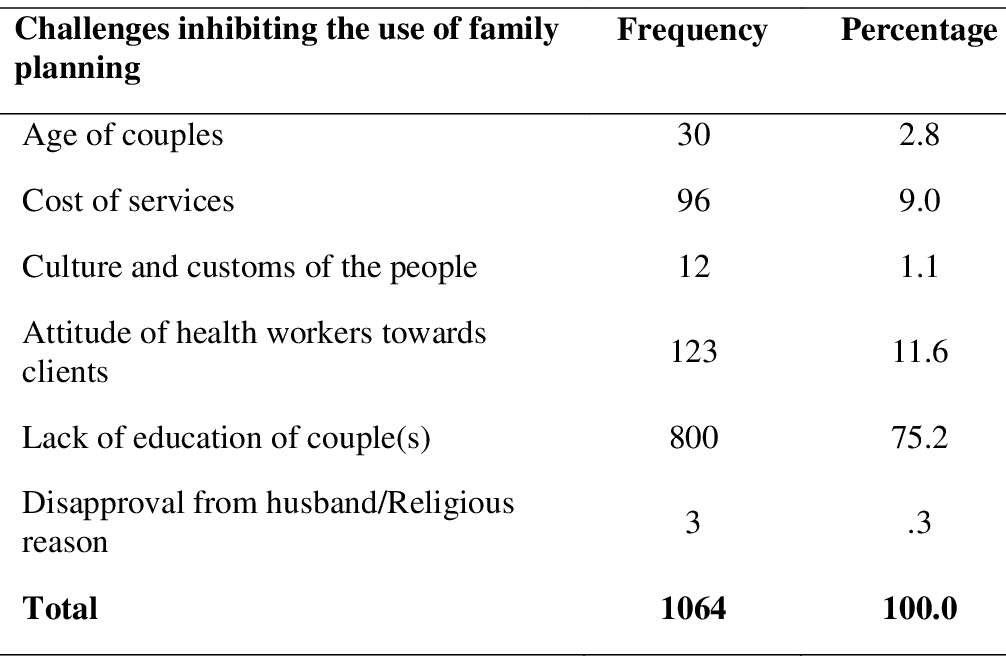
Source: Author’s Field Survey, 2022 In Figure 6, respondents were asked the proximity of their family planning centres from their houses. Majority (76.6%) of the respondents said their family planning centres were not so or very close to their place of residences, 11.6% said it was very far from their houses, 7.9% said they don’t know, 3.7% said it was far from their house and 0.3% said it was very close to their house. These findings imply that since most of the spouses live quite far away from where the very few available family planning clinics are located, it makes it cumbersome for spouses and/ or couples to access such services. Table 3: Distribution of respondents on factors inhibiting the use of contraceptives
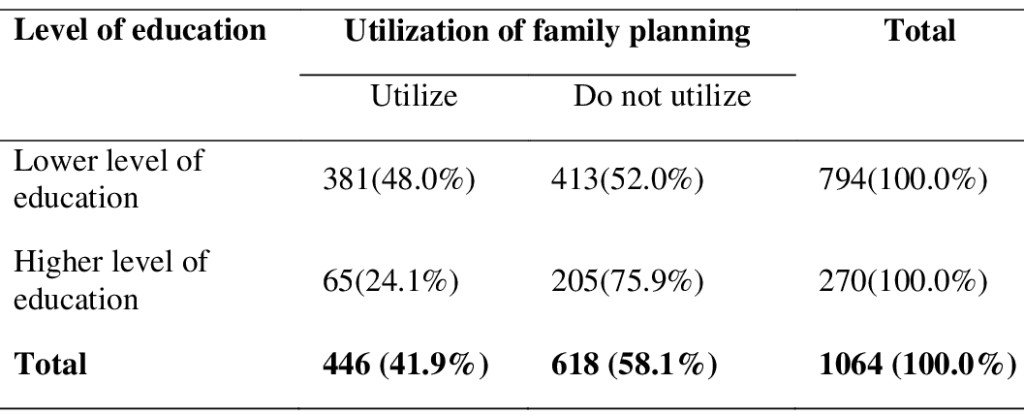
Source: Author’s Field Survey, 2022 Entries displayed in Table 3 revealed the challenges inhibiting the utilization of family planning services by respondents. Out of the 1064 respondents who were sampled for this study, majority (75.2%) said lack of education of spouse(s) inhibits the use of family planning, 11.6% mentioned attitude of health workers towards clients, 9.0% said cost of services, 2.8% mentioned the age of spouses, 1.1% mentioned culture and customs of the people and 0.3% said disapproval from husband/religious reason. This finding implies that amidst the numerous challenges inhibiting the use of family planning methods, lack of education of spouses’ poses more threat. Decision Rule: In the application of Chi-square (χ2) for the test of hypotheses, the following rule was applied: Reject the null hypotheses if the calculated value of the test statistics is greater than the table value. Hypothesis one Null hypothesis (H0): Spouses with higher level of education are not more likely to utilize family planning services than those with lower level of education. Substantive hypothesis (H1): Spouses with higher level of education are more likely to utilize family planning services than those with lower level of education. Table 4: Percentage distribution of respondents on utilization of family planning by level of education
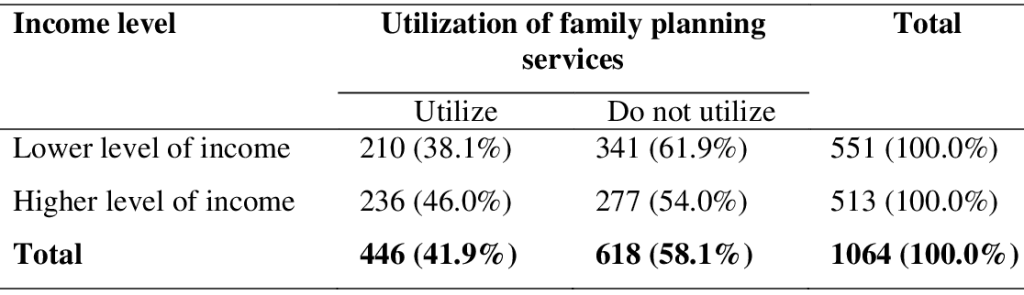
Source: Author’s Field Survey, 2022 To test hypothesis one, the Chi square test result showed that the computed χ2 is 47.314 while the critical/table χ2 value is 3.841 and df= 1. The test also showed that there is a statistically significant relationship (P <.000) between education and the utilization of family planning services. From the decision rule, since the chi-squared calculated (47.314) is greater than the chi-squared tabulated (3.841) we accept the substantive hypothesis which stated that spouse with higher level of education are more likely to utilize family planning services than those with lower level of education, while the null hypothesis which stated that spouse with higher level of education are not more likely to utilize family planning services than those with lower level of education is hereby rejected. Hypothesis two Null hypothesis (H0): Spouses with higher level of income are not more likely to utilise family planning services than those with lower income level. Substantive hypothesis (H1): Spouses with higher level of income are more likely to utilise family planning services than those with lower income level. Table 5: Percentage distribution of respondents on utilization of family planning services by income level
χ2=6.795, df=1, N=1064, p< .009 Source: Author’s Field Survey, 2022 To test hypothesis three, the Chi square test result shows that computed χ2 is 6.795 while the critical/table χ2 value is 3.841 and df=1. The test shows that there is a statistically significant relationship (P <.009) between income and utilization of family planning services. From the decision rule, since the chi-squared calculated (6.795) is greater than the chi-squared tabulated (3.841) the substantive hypothesis which states that spouse with higher level of income are more likely to utilize family planning services than those with lower level of income is hereby accepted while the null hypothesis which states that spouse with higher level of income are not more likely to utilize family planning services than those with lower level of income is hereby rejected. Discussion of Findings Reachability of Modern Contraceptives/Family Planning Services Being informed about a family planning service is good but the availability of these services makes it important for respondents to easily access these services. Findings from this study revealed that majority (50.3%) of the respondents said that family planning services was not available in their locality. This finding is in congruent with what Ahmed, Shokai, Abduelkhair, and Boshra (2015) found. Concerning the availability of family planning services, people in Jelhak mentioned that family planning services do not exist. It was observed that there was only one health centre which provides medical services in addition to selling pills with very low rates. Furthermore, this finding found that a little less than majority (41.8%) of the respondents said counselling of clients for appropriateness of methods and provision of variety of contraception were the available family planning services. This finding has a slight dissimilarity with that of Ahmed, Shokai, Abduelkhair and Boshra (2015). According to them, women and men in Jelhak and Renk had good knowledge about traditional and modern methods of family planning and poor knowledge about contraceptives. Injectable contraceptives rated the lowest of all while condoms were well known but remains socially unacceptable. Utilization of Modern Contraceptives/Family Planning Services In terms of the utilization of family planning, majority (54.5%) of the said they had no access to family planning services hence they cannot utilize it. Also, this study found out that despite the level of awareness of family planning services available in Kogi State, majority (58.1%) of the respondents said they don’t utilize family planning services. When asked the reasons for not utilizing family planning services, majority of the respondents said family planning services have harmful health side effects while another significant majority said it was against their religion. Similar finding by Etokidem, Ndifon, Etowa and Asuquo (2017) revealed that 56.0% of their study respondents indicated that their religious belief hinders their utilization of family planning services. Another striking finding is that 52.5% of the study respondents said they were not currently utilizing family planning services. This is in contrast to the finding of Ushie, Otu and Undelikwo (2014) in Cross River State. Ushie, Otu and Undelikwo (2014) found that 61.3% of their respondents were currently using one form of family planning method or another. Factors Influencing the Uptake of Modern Contraceptives/Family Planning Various factors influence the utilization of family planning services. From this study, it was found that accessibility, cost, proximity, culture and religion were all the reasons why people utilise or do not utilize family planning services. Again, FGD from Kogi-East revealed that place of residence was an influencing factor for the utilization of family planning. According to a participant, “the family planning centre is quite far from my place of residence and coupled with the hard economic state of things in our state, I find it hard making it to the family planning centre for the use of the services therein”. This finding has similarities with that of Gaetano, Lutuf, Zaake and Annika (2014) who, in their study, revealed that although most people were aware of the benefits of family planning services, they however complained that it was difficult to access family planning services because these services were provided by health facilities that were far from their homes. Education is a major factor in influencing the use of family planning method; majority (75.2%) of the respondents indicated that lack of education inhibits the utilization of family planning. This Finding is slightly similar to that of Apanga and Adam (2015). Apanga and Adam (2015) in their study revealed that lack of knowledge and misconceptions about family planning have been strongly linked with non-use of family planning methods. Conclusion This study investigated the reachability and use of modern contraceptives among spouses in Kogi State, North-Central, Nigeria. The use of modern contraceptive is important in preventing maternal and neonatal deaths; hence, its availability and accessibility cannot be overemphasized. This study provides facts to demonstrate that even though there is a good knowledge of modern contraceptive among spouses in Kogi State, it does not inevitably increase the reachability and use of modern contraceptive since the spouses indicated that they had no access to these services and that it was not available. It is therefore crucial to enlighten people on where to find these services and how to utilize these services. This will help spouses utilize family planning services. Husbands should be fully active in family planning decisions. Women should not be made to go through this stage alone. Both husband and wife should take decisions of family planning services. To this end, the government, organizations, international bodies, community leaders, institutions, health workers and the general public should quickly rise to their distinct responsibilities in providing relevant information about family planning services. Recommendations Based on the findings, the researcher recommends the following to guide the government, religious leaders, organizations, institutions, health care providers, sociologists, all spouses and the general public in addressing issues on the reachability and uptake of modern contraceptives. The recommendations are:
References Adansi-Pimpim, G., Kwafo, S. K., & Garchiner, C. (2016). Family planning and maternal and child health: The experience in Ghana: Developments in family policies and programmes in Africa. Legon, Ghana. (RIPS), 319-350. Adeleye, O. A., Akoria, O. A., Shuaib, Z. O. & Ogholoh, O. D. (2010). Barriers and Knowledge of benefits regarding family planning methods among women attending antenatal clinics in a southern Nigerian community. Asian Journal of Medical Sciences, 2(4):190-194. Adinan, B. S. (2013). Awareness and practices of family planning in the WA Municipality. European journal of business and management. Vol. 5, No. 19, 2013: 132-143. Ahmed, W., Shokai, S. B., Abduelkhair, I. H., &Boshra, A. Y. (2015). Factors Affecting Utilization of Family Planning Services in a Post-Conflict Setting, South Sudan: A Qualitative Study. AIMS public health, 2(4), 655–666. doi:10.3934/publichealth.2015.4.655 Ashimi, A. O., Amole, T. G., Ugwa, E. A., &Ohonsi, A. O. (2016). Awareness, Practice, and Predictors of Family Planning by Pregnant Women Attending a Tertiary Hospital in a Semi-rural Community of North-West Nigeria. Journal of Basic and Clinical Reproductive Sciences, 5(1), 6-11. Apanga, P. A., &Adam, M. A. (2015). Factors influencing the uptake of family planning service in the Talensi district, Ghana. Pan Afr Med J, 2(1), 10doi:10.11604/pamj.2015.20.10.5301. Bankole, A. (2008). Barriers to safe motherhood in Nigeria. New York: Guttmacher Institute. Bankole, B. (2009). Mass Media and reproductive behaviour in Africa. Calverton, Maryland: New York. Bongaarts, J. & Bruce, J. (1995). The causes of unmet need for contraception and social content of services. Stud FamPlann. 1995, 26 (Suppl 2): 57-75. Bradley, S., Hilary, M. S., & Shane, K. E. K. (2009). Levels, trends and reasons for contraceptive discontinuation. DHS Analytical Studies. 2009, 20: 27-37. Berghella, V. Buchanan, E. & Pereira, L. et al. (2010). Preconception care. Obstet Gynecol Surv. Feb; 65(2):119-31. Campbell, M., Nuriye, N. S., & Malcolm, P. (2006). Barriers to fertility regulation. A review of the literature. Stud Fam Plann. 2006, 37 (Suppl 2): 87-98 Centres for Disease Control and Prevention. (1999). Achievements in public health, 1900–1999: Family planning. MMWR Weekly. 1999 Dec 3; 48(47):1073-80. Retrieved on the 21/03/2022 from: https://www.cdc.gov/mmwr/preview/mmwrhtml/ mm4847a1.htm. Cochran, S. (1977). Sample Size Determination, New York: John Winley & Sons, Inc, New York. Colombia Demographic Health Survey (2005). Colombia 2005: Results from the demographic and health survey. Studies in family planning, population commission, Vol. 38, No. 1 (Mar; 2007), pp. 55-60. Darroch, J. E., Gilda, S., & Haley, B. (2011). Contraceptive technologies: Responding to women’s needs. 2011, New York: Guttmacher Institute. Gavin, L. Moskosky, S. Carter, M. et al. (2014). Providing quality family planning services: recommendations of CDC and the US Office of Population Affairs. MMWR Recomm Rep;63(No. RR-04). Gavin, L. & Pazol, K. (2016). Update: Providing Quality Family Planning Services –Recommendations from CDC and the U.S. Office of Population Affairs, 2015. MMWR Morb Mortal Wkly Rep; 65:231–234. DOI: http://dx.doi.org/10.15585/ mm6509a3. Gipson, J. Koenig, M. & Hindin, M. (2008). The effects of unintended pregnancy on infant, child and parental health: A review of the literature. Studies in Family Planning; 39(1):18-38. Guttmacher Institute. (2010). Sub-Saharan Africa: Facts on investing in family planning and maternal and newborn health. New York: Guttmacher Institute & UNFPA. Retrieved on the 13/04/2022 from http://www.unfpa.org/webdav/site/ global/shared/additup/factsheet_aiv_africa_ en.pdf. Guttmacher Institute. (2014). In Brief: Facts on Publicly Funded Contraceptive Services in the United States. New York, NY: Retrieved on 22 March, 2022 from: https://www.guttmacher.org/pubs/fb_contraceptive_serv.html. Hill, K., You, D., Inoue, M., &Oestergaard, M. Z. (2012). Technical Advisory Group of United Nations Inter-Agency Group for Child Mortality Estimation. PLoS Med, 9(8): e1001303. Iniabasi, N. I & Anthonia, A. (2013). Adolescents and utilisation of family planning services in rural community of Nigeria. Journal of research on humanities and social sciences. www.iiste.org. Vol.3, No. 1. pp. 112-132. Kabagenyi, A. Jennings, L., Reid, A., Nalwadda, G., Ntozi, J., &Atuyambe, L. (2014). Barriers to male involvement in contraceptive uptake and reproductive health services: a qualitative study of men and women’s perceptions in two rural districts in Uganda. ReprodHealth.11(1):21. KOSEEDS (2015). Kogi State Economic Empowerment and Development Strategy: A Bridged Version. Kogi State Ministry of Budget and Planning 2015.Lokoja, Kogi State, Nigeria. Lawrence, E. B. & David, E. (2008). Rationality. The New Palgrave Dictionary of Economics. 2nd Edition. Monjok, E., Andrea, S., John, E. E., & Essien, J. E. (2010). Contraceptive practices in Nigeria: Literature review and recommendation for future policy decisions. Open access journal of contraception, 1:9-22. Nabila, J. S. (2014). “The Ghana national family planning programme and national development” paper presented at the National conference on population and national reconstruction. University of Ghana, Legon, April 7-10. National Population Commission (2006). Federal Republic of Nigeria. Official Gazette, 94,178-198. National Population Commission (Nigeria) & ICF Marco. 2009. Nigeria Demographic and Health Survey 2008. Abuja, Nigeria: National Population Commission and ICF Marco. Nigeria Demographic and Health Survey (NDHS) 2008. National population commission, Federal Republic of Nigeria. Abuja, Nigeria & ICF Macro. Calverton, Maryland, USA. November 2009. NPC (2009). Kogi State Priority Table Vol. NPC 2006 population and housing census of the Federal Republic of Nigeria. Okeowo, T. A., & Olujide, M. G. (2014). Attitude, knowledge and utilization of family planning methods among rural women in Ogun State, Nigeria. Agrosearch, 14 (1), 39-53. Paschal, A. A., & Matthew, A. A. (2015). Factors influencing the uptake of family planning services in the Talensi District, Ghana. Pan Afri Med J. 2015; 20: 10. doi: 10.11604/Pamj.2015.20.10.5301 Rugendo, M. M., &Maseno University (2015). Assessing utilisation of family planning services among women of reproductive age (15-49 Yrs) in North Kanyabala sub-location, Homabay sub-county. Journal of Biology, Agriculture and Healthcare.Vol. 5, No. 7, 2015. www.iiste.org. Retrieved on 20th May, 2016. Samuel, E. (2010). Human Sexuality & Family Health Education, Nsukka, Afro-Orbis Publishers Limited. Sedgh, G., Rubina, H., Akinrinola, B., & Susheela, S. (2007). Women with an unmet need for contraception in developing countries and their reasons for not using a method. Occasional Report. New York: Guttmacher Institute Semachew-Kasa, A., Tarekegn, M., & Embiale, N. (2018). Knowledge, attitude and practice towards family planning among reproductive age women in a resource limited setting of Northwest Ethiopia. BMC research notes, 11(1), 57.doi:10.1186/s13104-018-3689-7 Sonfield, A. Hasstedt, K. & Gold, R. B. (2014). Moving Forward: Family Planning in the Era of Health Reform, New York: Guttmacher Institute. Uganda Bureau of Statistics (UBOS) and ORC Macro (2001). Uganda Demographic and Health Survey 2000–2001. 2001, Calverton, Maryland, USA: UBOS and ORC Macro. Ushie, M. A., Otu, J. E., & Undelikwo, V. A. (2014). A comparative analysis of fertility differentials in Cross River State. Dev Country Study, 4(1), 36-40. Westoff, C. F. (2011). Unmet need at the end of the century. DHS Comparative Reports No.1. Calverton, Maryland: ORC Macro. World Health Organization (2010). World health statistics: (Geneva: World health organization. World Health Organization (WHO) (2013). Family planning fact sheet. Retrieved on the 26/03/2022 from http: //www.who.int/mediacentre/factsheets1to351/en/pdf. |
||||
|
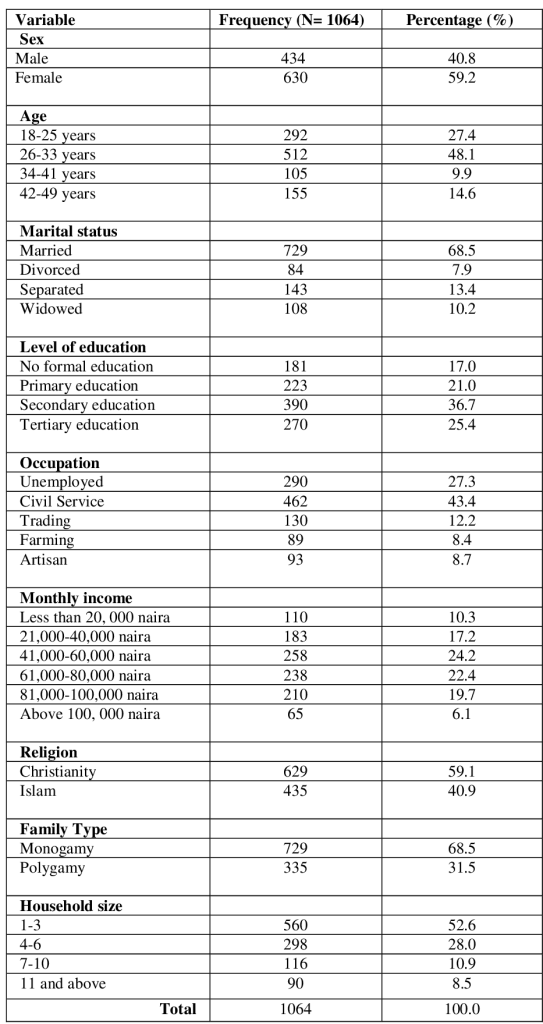
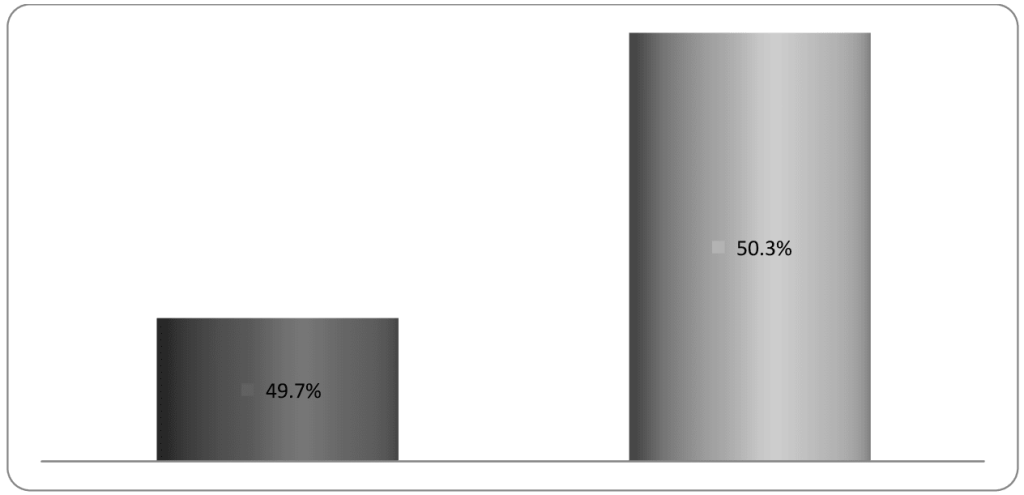
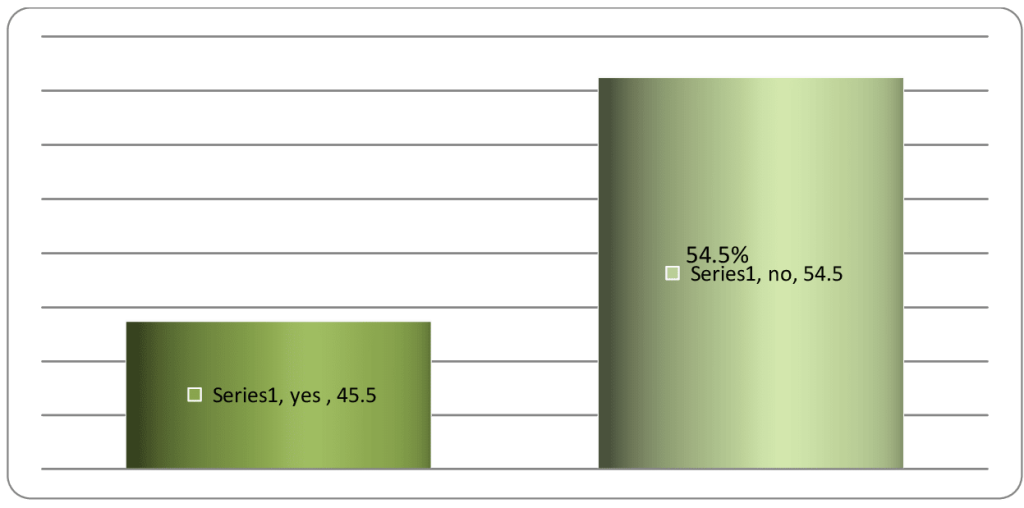
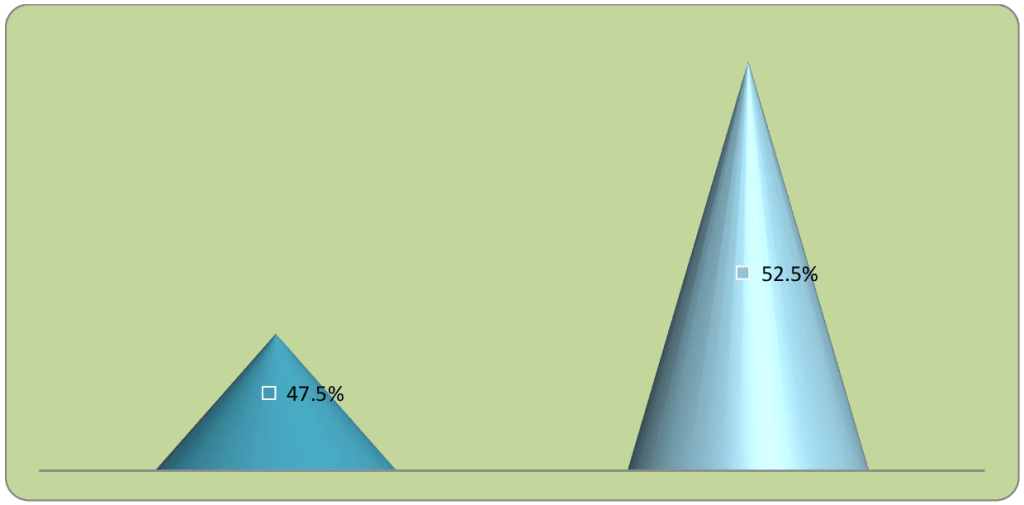
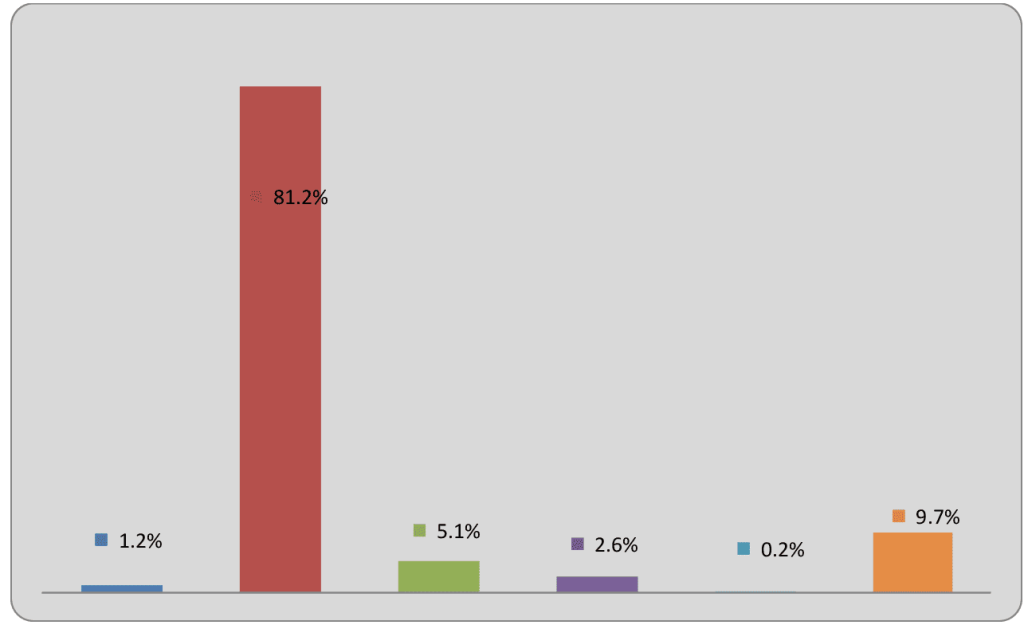
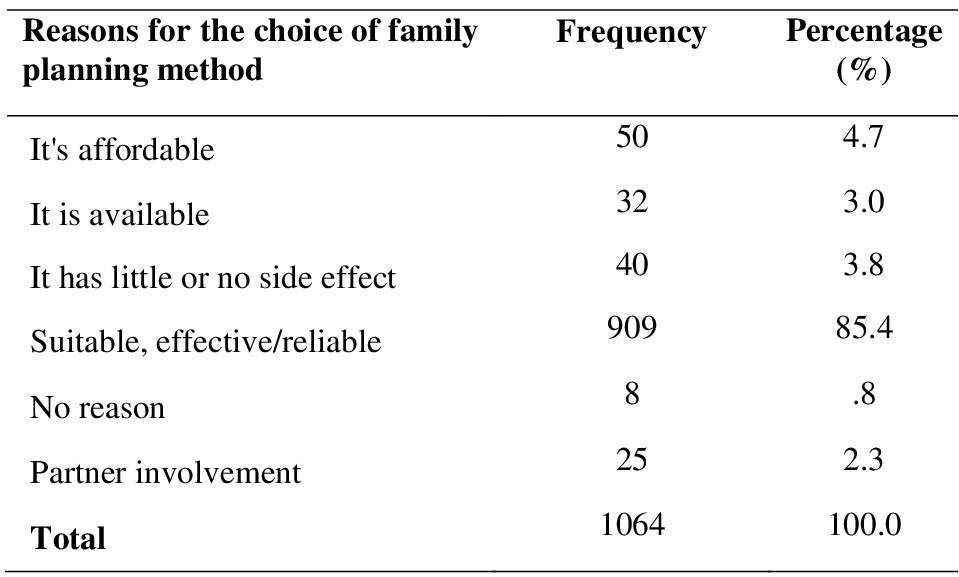
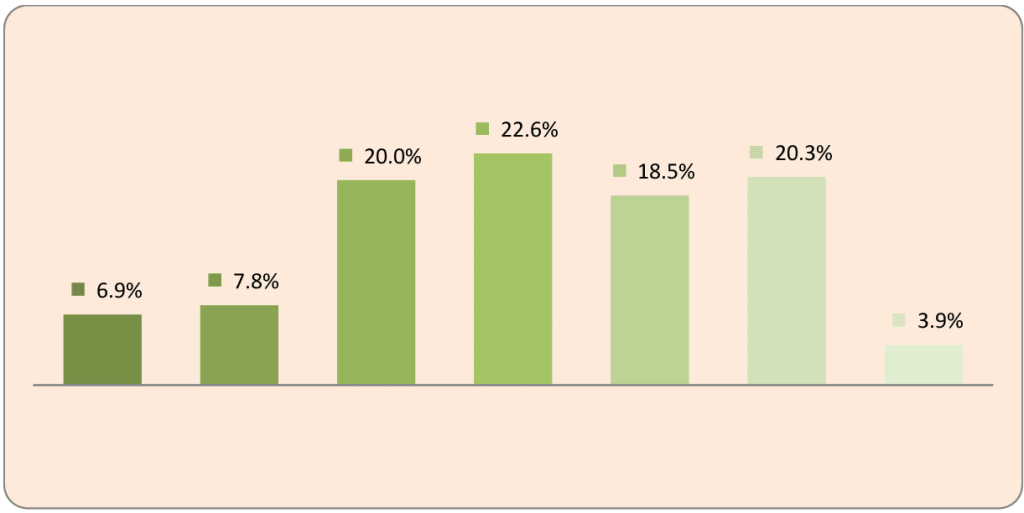
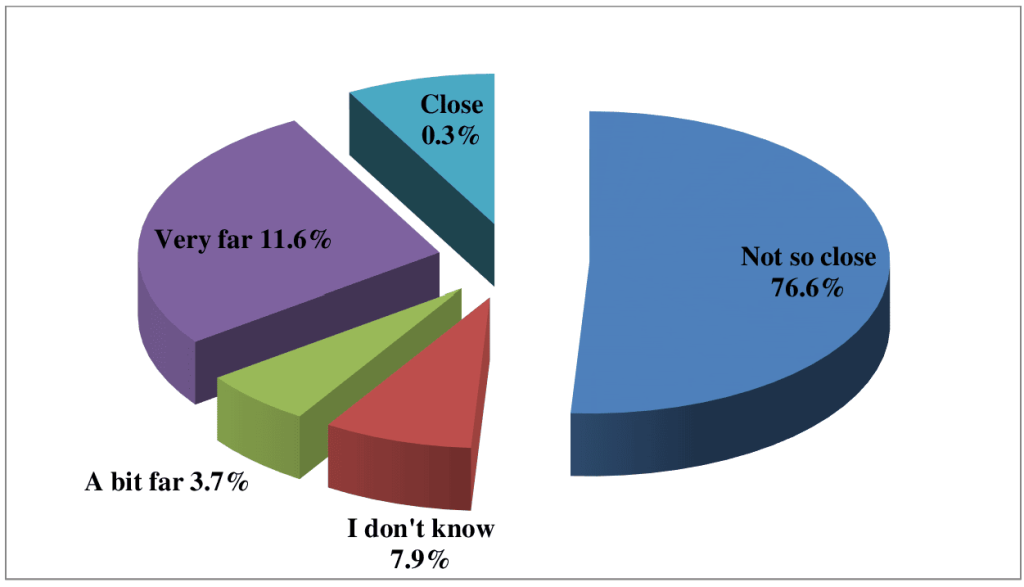 Figure 6: Distribution of Respondents on proximity to family planning centre from their house
Figure 6: Distribution of Respondents on proximity to family planning centre from their house